Report Published January 21, 2014 · Updated January 21, 2014 · 9 minute read
Reduce Unnecessary Radiological Exams
David Kendall & Elizabeth Quill
Takeaways
Radiological exams (“imaging”) are often unnecessary, increasing health care costs and exposing patients to dangerous radiation.
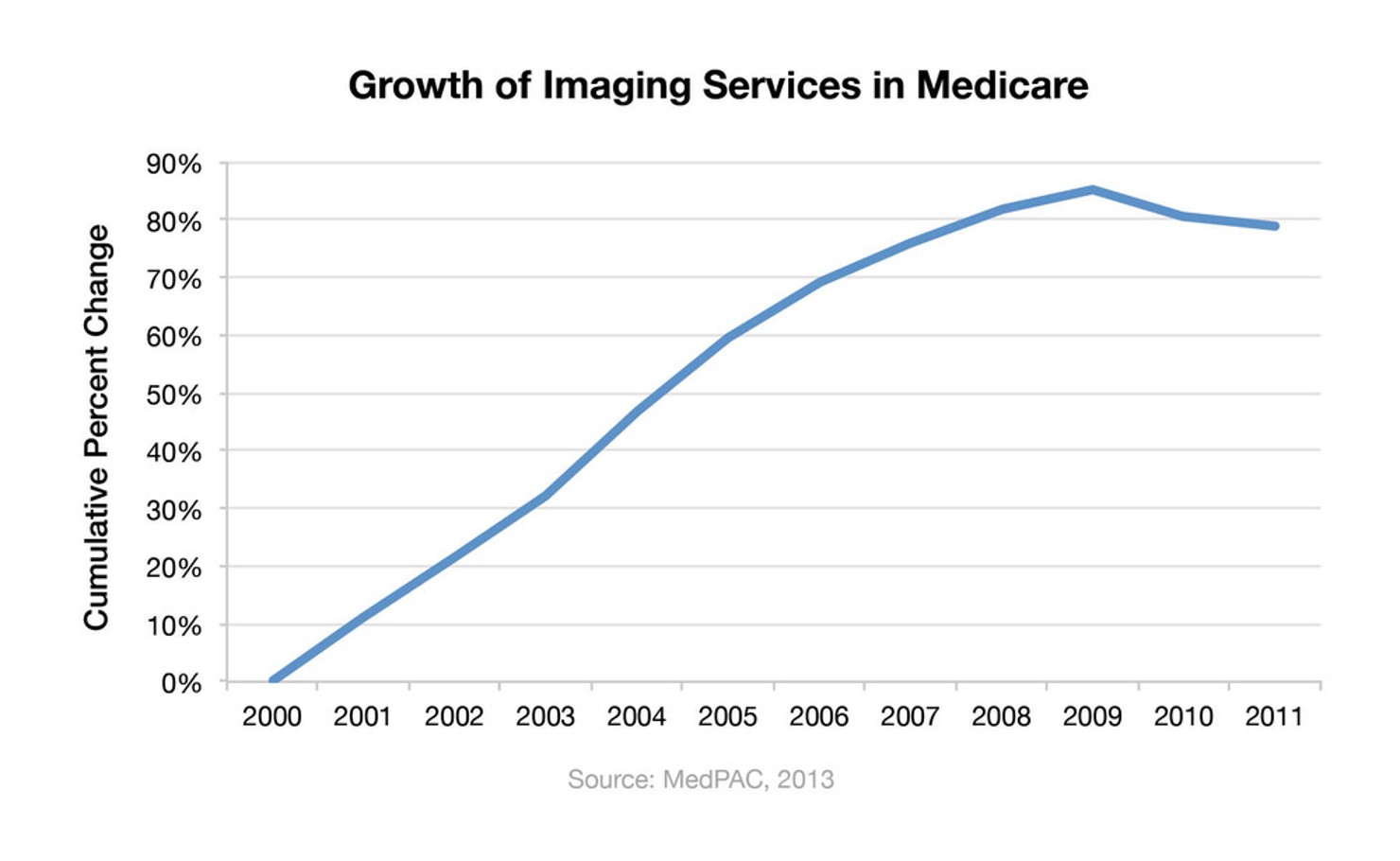
- Between 2000 and 2011, imaging volume in Medicare increased by over 80%.
- Private health plans in Medicare have had success reducing cost and the risk of cancer in patients by requiring providers to receive preauthorization for imaging and providing them with decision-support tools for ordering imaging.
- Medicare’s imaging rate in its public plan is 8.5% higher than in the private plans, and it could save millions of dollars, if not billions, by adopting a preauthorization policy for imaging.
Many of the radiological exams (“imaging”) performed are unnecessary, increasing health care costs and exposing patients to dangerous radiation. By requiring providers to receive pre-authorization for imaging and providing them with decision support, Medicare could reduce costs and cancer in patients.
Current behavior: Doctors may order radiology exams without considering medical needs or the risk of radiation to patients.
New behavior: Doctors order imaging only as needed, consider the risk to patients individually, and use science-backed guidelines to check their decisions.
How to change behavior: Medicare and other health plans would pre-authorize imaging to ensure effectiveness and safety to patients.
What’s Wrong?
In the past decade there has been significant growth in radiological exams that create diagnostic images of the body, such as magnetic resonance imaging (MRI), computed tomography (CT), and myocardial perfusion imaging (nuclear studies or MPI). Cumulative growth of imaging services per beneficiary from 2000 to 2009 was 85% and outpaced growth in all other categories of physician services except laboratory tests1. In 2010 and 2011, imaging volume in Medicare declined slightly; however, it is still up by over 80% since 2000.2
Many of these services are not clinically appropriate. A study by the American College of Cardiology Foundation (ACCF) and United Healthcare found that 14% of the services performed at the practices studied were inappropriate and 15% were of “uncertain appropriateness.”3 Another study found that nearly 30% of Medicare beneficiaries with uncomplicated lower back pain received an imaging service within 28 days, even though imaging is rarely indicated in the absence of complications.4
The path of least resistance for physicians is to order imaging tests, which either they perform themselves or refer to a radiologist. Determining which patients do not need imaging often requires an extensive and lengthy review of research, which is a huge hurdle for most physicians.5 But even radiologists, who are more likely to know the research, do not act as gatekeepers by saying no to unnecessary exams; instead, they are often expected to perform the exam regardless of their opinions.6
In fact, some surgeons will not see a patient until he or she has a CT scan.7
Physicians also face the threat of a lawsuit if they do not order a test and a patient subsequently has a major health care problem. In other cases, physicians may err on the side of ordering tests when they own their own radiological equipment and can benefit financially from ordering the test. Patients themselves play a role in unnecessary testing because they have come to expect imaging as a hallmark of good medical care and don’t question the need for them.8
All of these problems start with the lack of knowledge about when imaging is not necessary. Keeping up with research and systematically incorporating it into the daily practice of medicine is a general problem for physicians.9
Even within narrow medical specialties, it is difficult to keep up with medical reports and suggested guidelines.10 Approximately 750,000 health care journal articles were published in 2010.11 With 37 specialty groups identified by the American Board of Medical Specialties, physicians from each specialty would have to read roughly 55.5 journal articles per day to stay informed.12 There is also little guidance for physicians on what constitutes the best and most accurate information.13 For those reasons, new research about medical effectiveness is often not incorporated into daily practice in a timely fashion.14 This information overload requires tools that will efficiently provide the information necessary to make the decision.
Behavioral Economics 101
Information overload refers to the over-abundance of information that can make it difficult to make a decision and can result in decision paralysis.
It is important to note that informing physicians of the costs of imaging, while helpful, will not curb overuse of imaging. One study provided physicians with the costs of the most frequently ordered imaging tests and produced no reduction in the number of imaging tests ordered.15 In addition to the unnecessary costs of such procedures, unnecessary tests can have harmful health effects. Radiation can cause damage to DNA, increasing a person’s lifetime risk of developing cancer. The estimated radiation exposure of an abdominal CT scan, for example, is 8 millisieverts (mSv), the equivalent of 400 chest x-rays.16 When these tests are used appropriately, the benefits outweigh the radiation risks, but when they are misused, they needlessly increase a patient’s radiation exposure. For example, a recent study found that more than 50% of abdominal CT scans may be unnecessary and dangerous for patients.17
What Can Fix It?
Unnecessary imaging can be reduced by requiring pre-authorization for such exams. Pre-authorization means that physicians ordering exams request that Medicare or a health insurance plan approve payment for the exam before performing it. The physician typically contacts a radiology benefit manager to ensure that the testing approach meets clinically proven guidelines established by the American College of Radiology and other medical societies.18 Those tests that do not meet guidelines would not be covered under a beneficiary’s benefits. Savings come from eliminating inappropriate testing and the use of lower-cost alternatives where appropriate.
Clinical decision support is another critical tool to help physicians weed out unnecessary imaging tests. It provides physicians with information about imaging exams that are specific to the patient they are treating. It takes all the research about imaging techniques and effectiveness and assembles it into a website where doctors enter information about a patient and receive scientifically-based recommendations. By using science-based guidelines from medical societies, decision-support tools avoid the problems documented in some clinical review programs that do not use established guidelines.19
The decision-support tool can also track a patient’s radiation exposure. They can alert a physician if a patient has had several images that increase the risk of cancer. The tools allow physicians to gather data for reviewing their own performance in choosing appropriate imaging services and keep decision-making in the hands of doctors.20
Clinical decision-support tools alleviate the decision-making challenges caused by information overload.
These two approaches—pre-authorization and clinical decision support—are blended together in a bipartisan, bicameral draft proposal by the Senate Finance Committee and the House Ways and Means Committee.21 For physicians ordering advanced imaging and echocardiogram services, Medicare would require physicians to consult a decision-support tool about the appropriateness of the test before payment is authorized. For physicians who regularly ordered imaging that fell outside the guidelines, Medicare would require their orders to be pre-authorized prior to any payment. Medicare would expand this approach to other areas of medicine where physician practices fall outside the guidelines.
Where Is It Working?
Prior authorization for advanced imaging services is used widely by employers and private health plans but has not been adopted across all of Medicare. A Cleveland health plan instituted a prior authorization program for advanced imaging studies after observing an annual 20% increase in utilization. After requiring prior authorization, the plan saw a large reduction in the growth rate of advanced imaging utilization, while having a denial rate of only 1.5%.22 A key factor in getting those results is the suite of web-based decision-support tools that quickly support doctors as they make evidence-based choices in imaging for each patient.
AIM Specialty Health, a highly focused benefit management company based in Chicago, Illinois, utilizes a decision-support tool within its Radiation Safety Program. It identifies patients who have had multiple imaging studies that are associated with hazardous radiation, prompts doctors when certain thresholds are reached, and provides alternatives to advanced imaging exams, such as ultrasound. The program reduced cumulative radiation exposure for impacted members by an estimated 38,000 mSv and reduced costs by $3.6 million through eliminating unnecessary procedures.23 AIM has achieved these results without sacrificing the quality of care for beneficiaries and without adding administrative burden to doctors. In just a few minutes, doctors can seek an authorization using a web-based platform specifically designed to be easy for doctors to navigate.
Through a Health Care Innovation Award from the Center for Medicare and Medicaid Innovation, the Altarum Institute, a nonprofit health systems research and consulting organization, is partnering with United Physicians and Detroit Medical Center Physician Hospital Organization to reduce unnecessary imaging services for beneficiaries in Southeastern Michigan. The program will establish a data-exchange system between primary care and imaging facilities to increase evidence-based decision-making among physicians for MRIs and CTs for certain conditions. The goal is to reduce CT volume by 17.4% and MRI volume by 13.4% over three years, resulting in a 17% reduction in imaging costs.24
Potential Savings?
The potential for savings is clear from private sector efforts. For example, Wellmark Blue Cross Blue Shield in Iowa and South Dakota has seen annual returns of at least three dollars for every on dollar invested in pre-authorization.25 Extrapolated nationwide, private sector experience suggests higher savings of $2 to $4 per beneficiary per month ($720 million to $1.4 billion annually), depending on program design.26
Medicare’s imaging rate is 8.5% higher in a public vs. private plan
— WellPoint
Federal savings from the proposal by the Senate Finance and House Ways and Means committees, however, are scored differently with the Congressional Budget Office projecting savings of less than $50 million a year.27 Yet, savings are still very much possible. Despite the recent declines in imaging rates, Medicare’s imaging rate is 8.5% higher than the rate for a similar group of patients in a private plan using pre-authorization in the Medicare Advantage program.28 Developing a prior authorization model for imaging in Medicare can also generate additional cost-savings by applying it to other highly standardized medical services that have widely-agreed upon medical guidelines, such as echocardiograms, sleep management, and specialty pharmacy services.

