Memo Published February 17, 2026 · 7 minute read
Why Republican Changes to Medicaid State-Directed Payments Miss the Mark

High hospital prices are one of the biggest reasons Americans pay so much for health care. This problem affects not just those with private insurance and Medicare but also Americans who rely on Medicaid. And to understand the sheer impact hospital prices have on the Medicaid program specifically, it’s critical to examine an obscure but rapidly growing arrangement called state-directed payments. While state-directed payments were created to improve access for Medicaid patients, recent policy changes have turned them into a powerful—and problematic—vehicle for enriching hospitals with little oversight.
Republicans’ recent tax and health care legislation, the One Big Beautiful Bill Act (OBBBA), enacted historic and devastating cuts to Medicaid. It also acknowledged the need to rein in state-directed payments. But instead of fixing the policy with precision, Republicans enacted changes as part of a larger effort that kicked millions off of Medicaid in order to pay for their massive tax cuts. Their approach with across-the-board cuts leaves key problems unresolved, exacerbates inequities between states based on expansion status, and shifts exorbitant health care costs onto working families.
In this memo, we explain what state-directed payments are, where past policy went wrong, what OBBBA changed, and how to better fix issues in the future.
What Are State-Directed Payments?
Most states deliver Medicaid benefits through private health plans called managed care organizations (MCOs). These health plans receive fixed payments from the states to providers in order to cover enrollees’ health care needs. While these base payments cover all necessary services, states supplement them with state-directed payments. These are additional payments that states provide to MCOs that flow to providers, mostly hospitals.
Historically, Medicaid has paid providers well below their costs. As a result, some providers in non-emergency settings would decline to treat Medicaid patients, limiting access to care. To correct this disparity, in 2016, the Centers for Medicare and Medicaid Services (CMS) authorized states to distribute payments directly to providers at Medicare reimbursement rates to help raise Medicaid reimbursement levels, particularly for hospitals treating large volumes of Medicaid patients. These payments were meant to address concerns about low Medicaid payment rates without requiring states to overhaul their base payment structures. This was done with the intention that better-compensated providers will increase access to care, especially for those communities with high rates of Medicaid enrollees.
However, a major shift occurred in 2024 when CMS issued a new rule allowing states to raise these supplemental payments, not just to Medicare levels, but to the average of what hospitals charge patients with private insurance. This practice had been in effect before the rule but on a case-by-case basis. Nationally, hospitals charge private insurers 254% of what Medicare is charged. In Florida, charges go as high as 346% of Medicare rates.
The growth of state-directed payments has been dramatic—and highly concentrated. In 2024, just 10% of state-directed payment arrangements accounted for 70% of total state-directed payment spending. For example, the state of Tennessee, which is dominated by the HCA Healthcare system, increased state-directed payments to give hospitals an additional $3.2 billion. Due to the new reimbursement rates and the lack of oversight, a small number of high-cost deals are driving the bulk of Medicaid’s supplemental hospital spending, often benefiting large hospital systems rather than the safety-net providers most in need.
Problems with State-Directed Payments Before OBBBA
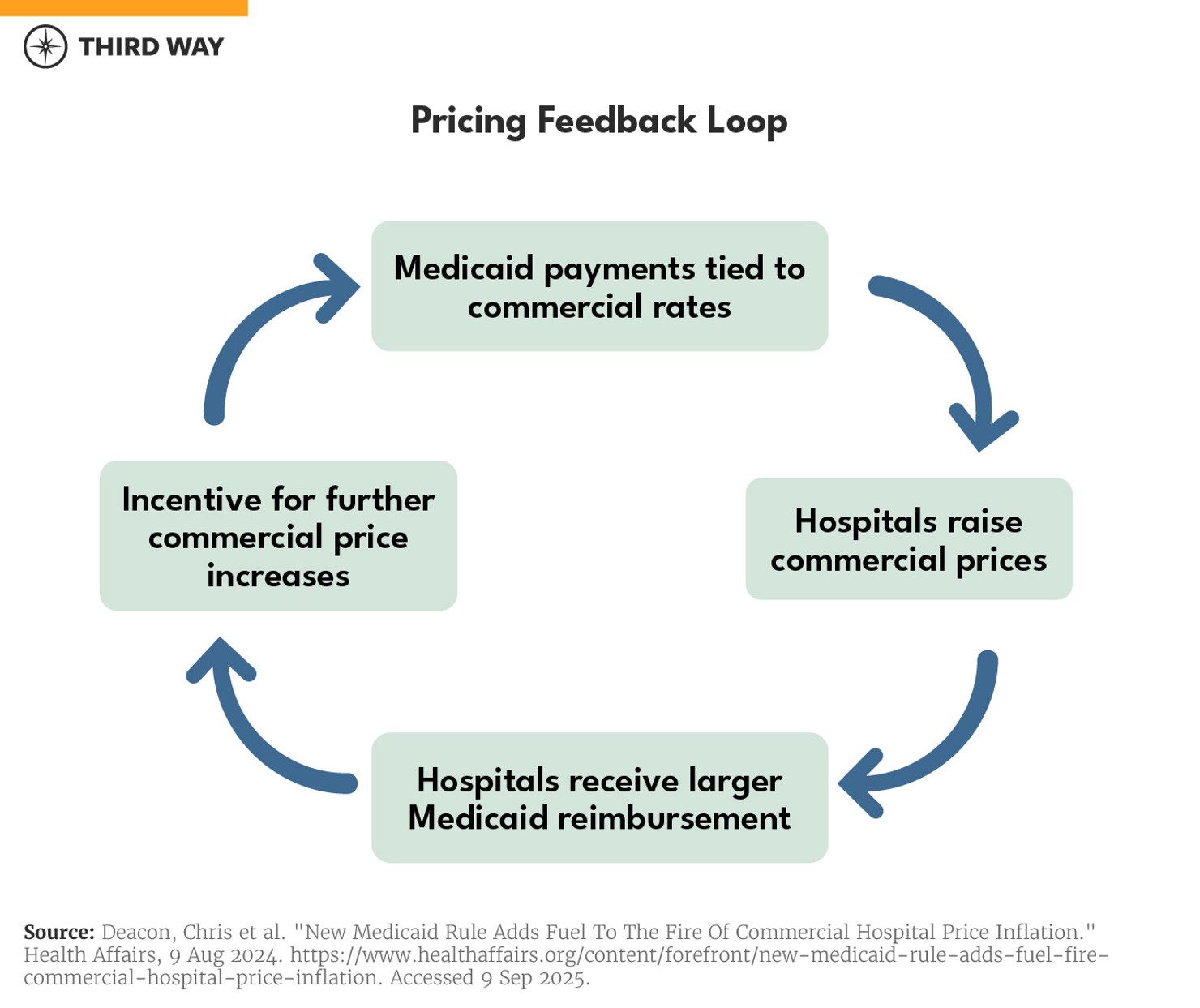
When state-directed payments in Medicaid are allowed to match commercial rates, it creates incentive to raise prices in the private insurance market. Hospitals financially benefit simply by inflating the price they charge private insurers so that they receive more in Medicaid payments, regardless of quality or value for patients. This pricing feedback loop then drives up costs across the health care system, ultimately harming the consumer.
Notably, commercial rates already far exceed the actual cost of delivering care. Nearly 75% of hospitals charge more than double Medicare rates, 32% charge more than triple, and 9% charge four times the Medicare rate. These markups don’t reflect higher quality or better outcomes—they reflect hospitals’ market power and ability to negotiate with private payers from a position of dominance.
That dominance stems from hospital consolidation. As major health systems acquire independent hospitals and physician practices, they reduce competition and expand their leverage over both private insurers and public payers. The new CMS policy exacerbates this problem by tying Medicaid reimbursements to these inflated commercial rates—essentially rewarding hospitals for consolidating and charging more.
The consequences are broad and problematic:
- Privately-insured patients face higher premiums, deductibles, and out-of-pocket costs to compensate for higher provider rates.
- Employers pay more to provide health benefits and put less in workers’ paychecks, which is especially hard on working-class families with tight budgets.
- State Medicaid programs face rising costs as hospital prices continue to climb, and Medicaid payments follow suit.
- Taxpayers—both state and federal—foot the bill, increasing strain on public budgets and reducing the ability to fund other health priorities.
OBBBA Changes
The Republican-passed OBBBA made significant changes to state-directed payments. First, it bars states from enacting new state-directed payments, effective immediately, that are above 100% of Medicare rates in states that expanded Medicaid as part of the Affordable Care Act and 110% of Medicare in non-expansion states. Then, beginning in 2028, existing state-directed payments must decrease by 10% a year until they reach 100% or 110%, depending on the state’s expansion status. Over the next 10 years, these changes will decrease federal Medicaid spending by $149 billion.
Issues with this Approach
While capping state-directed payments is a step in the right direction, the bill’s overall approach is flawed. There are four primary issues:
First, the new law encourages states to not expand Medicaid. While the pause on new state-directed payments applies to all states, mandatory decreases only apply to states that have expanded Medicaid. States should be incentivized to expand their Medicaid programs—not the other way around, especially when there is a coverage gap of 1.4 million Americans.
Second, changes to Medicaid should not be paired with policies that kick people off their coverage. Broadly, OBBBA’s reforms to Medicaid are going to result in 10 million people losing their coverage. The consequences will leave rural and safety-net hospitals worse off, resulting in a drastic rise in uncompensated care and a sicker population.
Third, the law widens the gap between have- and have-not hospitals. Rather than enact universal limits to state-directed payments, it would have been far more productive to create distinctions between hospitals based on the communities they serve and ensure supplemental payments within Medicaid work together. Hospitals in rural and low-income communities should have more flexibility with Medicaid reimbursement, while wealthier hospital chains should not. For example, a better approach would be to permit all states, regardless of expansion status, to have base payments for independent hospitals located in rural and low-income communities up to 150% of Medicare, accounting for each hospitals’ financial status, with all other hospitals at 110% to 130% of Medicare, for both fee-for-service and managed care.
Republicans may claim their newly created slush fund better targets hospitals in need than state-directed payments. However, as we’ve previously written, this fund is a Band-Aid on a giant self-inflicted wound that lacks any targeting mechanisms and is vulnerable to political abuses.
Finally, health care reforms should not be used to give tax cuts to the rich. Any changes to health care that reduce federal spending should be used in a fiscally responsible way—supporting other high-value care, reducing the nation’s deficit, or supporting critical investments. Instead, the bill as a whole increases the deficit by $3.4 trillion over the next decade.
Conclusion
State-directed payments were intended to increase access to care in Medicaid by keeping providers solvent—not drive-up costs, enrich big hospital systems, or widen inequities. The Republican approach in OBBBA acknowledges the problem but solves it in the most regressive way possible: by slashing Medicaid, preserving the worst abuses, and using the up-front savings for tax cuts.
If Congress wants to rein in hospital prices and make Medicaid sustainable, it must act with precision—not ideology. We need targeted reforms that close loopholes, improve care for all communities, and put patients first.
